Pneumothorax is the collection of air between the lung membranes in the chest cavity. Some people have air accumulation on the surface of the lung, especially in the upper part, which can be congenital.
Pneumothorax occurs spontaneously or otherwise due to the bursting of these bubbles. The air we breathe passes through the lungs, leaks into the pleural space, accumulates, and causes the lungs to deflate.
When the patient does not use the lung on the deflated side, the patient usually presents with chest pain. Sometimes they have complaints such as cough and shortness of breath.
There are three types of pneumothorax;
1. Spontaneous Pneumothorax
- It occurs due to the spontaneous bursting of bubbles, which we call blebs.
- This type of pneumothorax is the most common type of pneumothorax.
- It usually occurs in young, tall, and thin people.
- It is more common in men.
2. Secondary Pneumothorax (due to a disease)
Pneumothorax occurs due to lung diseases, such as emphysema, pre-existing giant balloons, pneumonia, or tuberculosis.
3. Pneumothorax resulting from medical intervention or after trauma (iatrogenic)
For Diagnosis of Pneumothorax:
- Patient's complaints,
- Physical examination and,
- Decreased respiration sounds are essential.
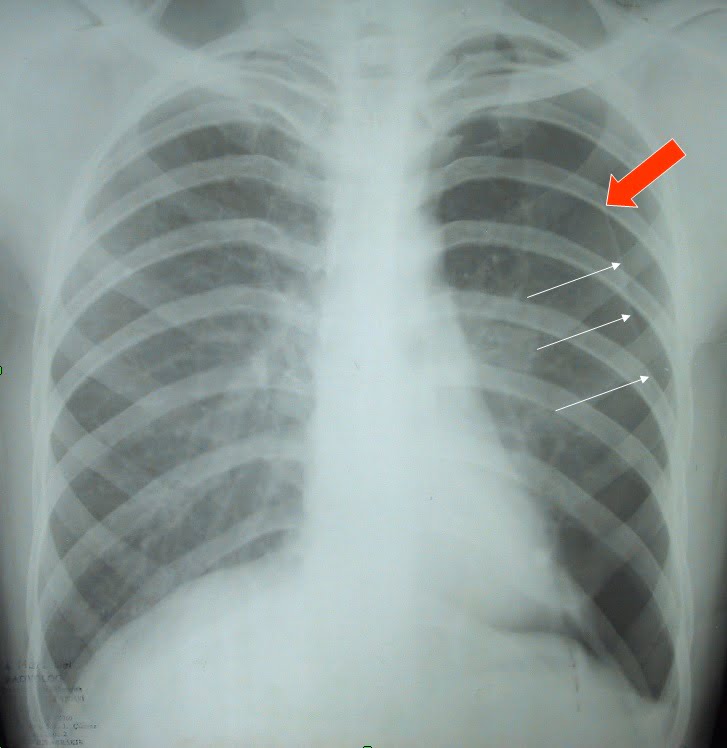
- Radiology: pneumothorax line..
- Direct chest X-ray: It provides the most practical diagnosis.
- Computed tomography of the thorax.
Pneumothorax can also occur due to trauma.
Pneumothorax Treatment : We aim to evacuate the air in the chest cavity and restore the lung's re-expansion to prevent its recurrence.
1. Chest Tube insertion (Tube thoracostomy)
- A catheter/drain is inserted under local anesthesia to evacuate the air between the pleura.
- It is an inpatient procedure.
- In general, within a few days, the air in the chest is evacuated, the lung expands, and the incision closes.
2. Observation and oxygen therapy
3. Evacuating the air with the needle, aspiration
4. Sometimes, surgery
When the pneumothorax recurs, we repair the burst bubble by thoracoscopy and closed surgery (VATS).Conditions requiring surgery:
- Recurrence of Pneumothorax
- Pneumothorax in both lungs
- The appearance of large balloon sacs in the lung
- Occupational reasons (such as pilots, divers)
Types of Surgical Methods
Open surgery / Axillary Thoracotomy: Performed with a 6-7 cm long incision made under the armpit with the help of a retractor between the three ribs.
Closed–Video Assisted Thoracoscopic Surgery (VATS): In this method, the camera is advanced through a single 1.5-2 cm incision (Single Port VATS) into the chest cavity. It is the safest operation method for patients.
In this VATS method, patients experience less pain, and the incision of the operation (2 cm) is much smaller and more aesthetic. Therefore, the patient returns to his everyday life quickly.
Pleurodesis: Sometimes, the pleura is partially removed so that the lung does not collapse again, the pleura is irritated, and an inflammation reaction is created to adhere to the lung.
The average length of stay in the hospital
- An average of 3 days (2-5) in a patient with a drain tube
- 4-5 days after open surgeries
- Closed surgeries – discharged two days after VATS surgeries

Does Pneumothorax Recur?
- The recurrence rate is 20-30% in patients who developed pneumothorax for the first time and recovered with a drain.
- The probability of this happening for the third time is 40-50% in people who have had pneumothorax twice and have been treated only with a drain placement.
- The recurrence probability of pneumothorax is 3-5% in people who have undergone surgery.
Tension Pneumothorax
Air accumulation in the pleural space during inhalation can not escape in expiration. These conditions increase pleural space pressure, and a tension pneumothorax occurs. Intrapleural pressure is positive, and a mediastinal shift develops; the vessels coming out of the heart are folded around themselves.

Clinically it presents as follows;
- Breathing difficulties and air insufficiency
- SRespiratory distress
- Tachycardia
- Tracheal deviation
- Unilateral loss of breath sounds
- Distention in neck veins
- Hypertympanism on percussion
- Cyanosis
*** The differential diagnosis of tension pneumothorax includes cardiac tamponade.
Follow-up: A lung CT is scanned after the operation to evaluate an underlying disease or other bubbles.